The thorax is a dynamic system acting as a ventilatory pump, formed by the spine, rib cage, and sternum, with the diaphragm as its base. Thoracic malformations in early childhood, termed volume depletion deformities, may cause devastating harm to thoracic function and requisite development, leading to life-threatening restrictive lung diseases. This serious disability has been defined as Thoracic Insufficiency Syndrome (TIS): the inability of the thorax to support normal respiration or lung growth. TIS is known to be associated with at least 28 pediatric diseases. Progressive TIS eventually reaches the point at which the thoracic engine of respiration is so damaged that respiratory insufficiency develops, with inadequate lung-gas exchange for normal clinical oxygenation needs, often requiring supplemental oxygen or more invasive support.
The major barrier to advances in the understanding and treatment of TIS is currently the absence of assessment technology to objectively characterize and measure the disease. Outcome assessment of thoracic and spinal surgery for TIS is currently relegated to radiographs or CT scans, with no ability to assess the effectiveness of the post-operative dynamic thoracic engine of respiration and its contribution to pulmonary function. Free-breathing thoracic dynamic MRI (dMRI) is the only viable imaging modality currently available to assess the thorax of these very sick patients with TIS. dMRI has great potential to clearly define quantitatively the dynamic biomechanical deficits of the thorax and abdomen and the response to treatment of young patients with TIS. The major hurdles currently preventing advances in TIS treatment include the lack of standardizable objective diagnostic measurement techniques that describe the 3D structures of the thoraco-abdominal region, the dynamics of respiration, and the changes that take place with growth.
The goal of this project is three-fold: (1) A normative database of dMRI images of normal children covering the entire pediatric age spectrum divided into several age groups will be built. Using the AAR technology, for each age group population anatomic models involving all key thoracic objects will be built. A comprehensive set of measurements to describe the object morphological (3D), dynamic (4D), and developmental (5D) parameters for each population group will be derived. The ensemble of images and the measurements is called a Virtual Growing Child (VGC) 5D model. (2) The effectiveness and utility of the VGC methodology in describing the outcome of TIS surgery will be tested based on existing pre- and post-operative data on a cohort of patients with Type I, II, or III volume depletion deformity. (3) The utility of the VGC approach in surgical planning will be tested on patients with Type II volume depletion deformity.
Towards the goals of the project, a method to construct an optimal 4D image representing the breathing thorax has been developed. A full free-breathing dMRI acquisition typically produces 2000-3000 slices over data gathered from 8-10 respiratory cycles. The 4D construction method selects from this set an optimal set of 200-300 slices constituting a 4D volume over one breathing cycle. We are in the process of validating this method via a 4D phantom which was created from 3D printing of a human lung model derived from an MRI data set of a normal volunteer. See the figure below.
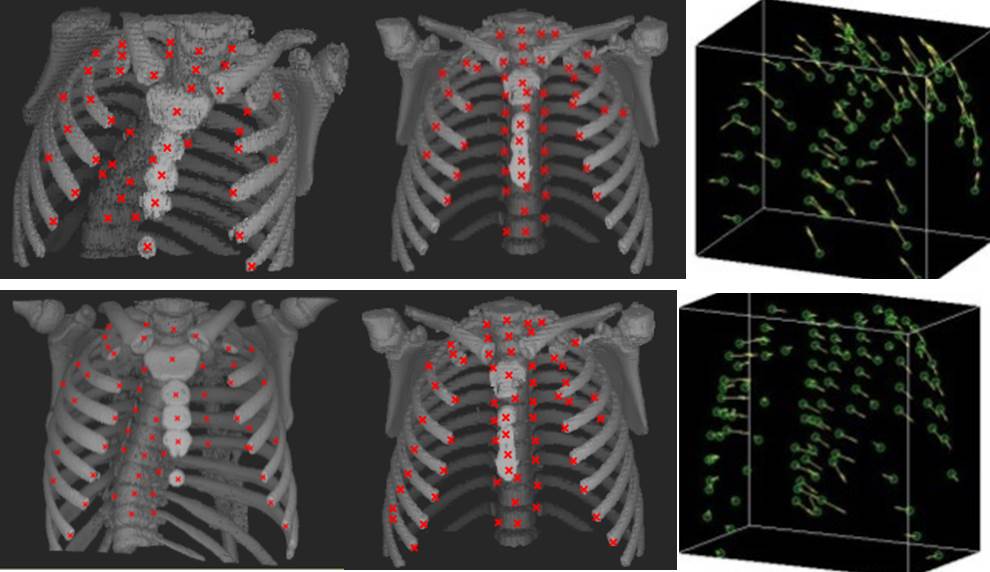
We are developing generalizations of the AAR approach to 4D data sets of the dMRI acquisitions. This also includes the development of techniques to study the major deformations a normal lung has to undergo to match it with a deformed patient lung. See the figure below. The top row of the figure shows (left to right): A 3D rendition of the skeletal structures of the pre-operative thorax of a 6 yr old patient with Type II TIS; a 3D rendition from a 7 yr old normal subject; and the deformation needed to match the patient structure to the structure of the normal subject. Post-operative results for the same patient 12 months after surgery are shown in the second row. These tools are being explored for planning optimal surgical intervention in patients with TIS.

References:
1. Tong Y, Udupa JK, Ciesielski KC, Wu C, McDonough JM, Mong DA, Campbell RM, Jr. Retrospective 4D MR image construction from free-breathing slice Acquisitions: A novel graph-based approach. Med Image Anal. 2017;35:345-59. doi: 10.1016/j.media.2016.08.001. PubMed PMID: 27567735; PMCID: PMC5099108.
2. Tong Y, Udupa JK, McDonough JM, Wileyto EP, Capraro A, Wu C, Ho S, Galagedera N, Talwar D, Mayer OH, Torigian DA, Campbell RM. Quantitative Dynamic Thoracic MRI: Application to Thoracic Insufficiency Syndrome in Pediatric Patients. Radiology. 2019;292(1):206-13. doi: 10.1148/radiol.2019181731. PubMed PMID: 31112090; PMCID: PMC6614911.
3. Tong Y, Udupa JK, McDonough JM, Wu C, Sun C, Qiu C, Lott C, Galagedera N, Anari JB, Mayer OH, Torigian DA, Cahill PJ. Thoracic Quantitative Dynamic MRI to Understand Developmental Changes in Normal Ventilatory Dynamics. Chest. 2020. doi: 10.1016/j.chest.2020.07.066. PubMed PMID: 32768456.
4. Udupa JK, Tong Y, Capraro A, McDonough JM, Mayer OH, Ho S, Wileyto P, Torigian DA, Campbell RM, Jr. Understanding Respiratory Restrictions as a Function of the Scoliotic Spinal Curve in Thoracic Insufficiency Syndrome: A 4D Dynamic MR Imaging Study. J Pediatr Orthop. 2020;40(4):183-9. doi: 10.1097/BPO.0000000000001258. PubMed PMID: 32132448; PMCID: PMC6426694.