Accumulation of body fat engenders increased risk and predisposition and adverse treatment outcome for many disease conditions including heart disease, diabetes mellitus, metabolic disorders, obstructive sleep apnea, certain lung diseases and their transplant surgery, and certain cancers. In practice, when fat composition in the body is quantified via images, fat area in just one slice imaged at the level of lumbar vertebrae L4-L5 is analyzed. This ubiquitous practice opens several questions: At what single slice anatomic location do the areas of Subcutaneous Adipose Tissue (SAT) and Visceral Adipose Tissue (VAT) estimated from a single slice best represent the corresponding volume measures? How does one ensure that the slices used for single slice area estimation from different subjects are at the homologous anatomic location? How can fat (SAT and VAT as separate components) be quantified throughout the body from low-dose CT and MRI images for each body region – neck, thorax, abdomen, and pelvis - separately?
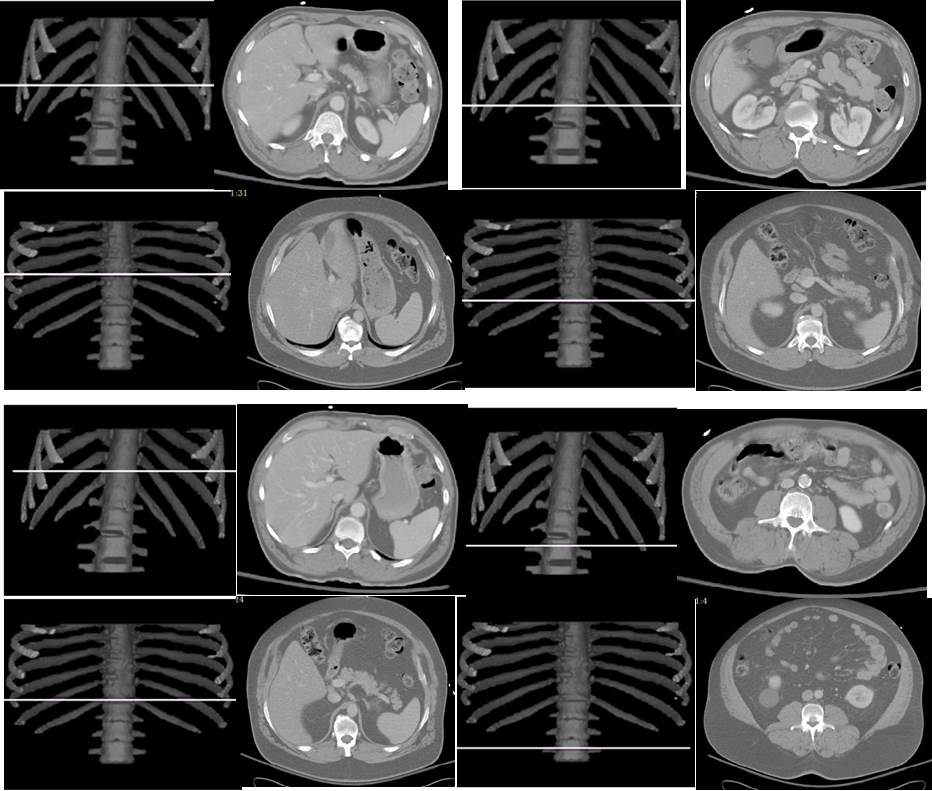
Based on AAR algorithms and the concept of standardized anatomic space, we are developing methods to answer the above questions. Our current results indicate that the best slice location (in terms of area-to-volume correlation) in the abdomen for SAT and VAT is not at L4-L5, but at thoracic vertebra T12 for SAT and L3-L4 for VAT. Similarly in the thorax the best locations are at T5-T6 for SAT and middle of the body of T9 for VAT. The following example illustrates best slice locations found without standardizing (top two rows – left column for SAT and right for VAT) and with standardized anatomic space (bottom two rows – SAT on left and VAT on right). The two rows represent two different subjects.